The Pharmacist
The Pharmacist (Pharmacist) is an open-access, peer-reviewed pharmacy journal, published half-yearly, as print and online by the The Pharmacist (Pharmacist) since 2025. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately upon acceptance of manuscript. In addition, the journal allows free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in journal. Manuscripts should be prepared in accordance with the author guidelines of the journal, w...
Integrative approaches for osteoarthritis: A collaborative review from ayurveda and modern pharmacy perspective
Osteoarthritis (OA) is a progressive, degenerative joint disorder characterized by cartilage degradation, synovial inflammation, and altered subchondral bone remodeling. Despite significant advances in pharmacotherapy, current management strategies often provide only symptomatic relief and are associated with long-term safety concerns. Integrative approaches that merge traditional Ayurvedic principles with contemporary pharmaceutical sciences offer a promising avenue for addressing the multifactorial nature of OA. This collaborative review synthesizes classical Ayurvedic conceptssuch as SandhigataVata, dhatukshaya, and amawith modern mechanistic insights involving inflammatory cascades, oxidative stress, matrix metalloproteinases, and chondrocyte apoptosis. The paper highlights evidence-based Ayurvedic interventions including Rasayana, Panchakarma, Sneha and Swedana therapies, herbal formulations (e.g., Shallaki, Guggulu, Ashwagandha), and diet-lifestyle regimens that target both systemic inflammation and tissue regeneration. Parallelly, contemporary pharmaceutical modalities such as Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), corticosteroids, viscosupplements, Disease-Modifying Osteoarthritis Drugs (DMOADs), and emerging nano-delivery systems are examined with respect to efficacy, safety, and mechanistic compatibility with Ayurvedic therapeutics. A central focus of the review is the scientific rationale for integrative careillustrating how Ayurvedic multi-target phytoconstituents can complement modern drug interventions through synergistic anti-inflammatory, chondroprotective, and immunomodulatory effects. The article also proposes a translational framework for collaborative research involving standardization of herbal drugs, bioactive compound profiling, pharmacokinetic/pharmacodynamic assessments, and clinical trial designs tailored for integrative OA management. Overall, the review advocates for a unified, evidence-driven approach bridging Ayurveda and modern pharmacy to enhance therapeutic outcomes, reduce adverse effects, and support personalized, holistic care in osteoarthritis.
1. Introduction
OA is a chronic, progressive, and debilitating musculoskeletal disorder marked by the structural and functional deterioration of synovial joints. Characterized by the erosion of articular cartilage, subchondral bone remodeling, and persistent low-grade inflammation, OA represents one of the most pressing global public health challenges of the 21st century. As the population continues to age and lifestyle-related risk factors escalate, the disease burden of OA is expected to rise significantly, demanding therapeutic innovations that extend beyond symptomatic relief and restore joint homeostasis through multi-dimensional interventions.[1][2]
1.1. Global prevalence and burden of osteoarthritis
Globally, OA affects hundreds of millions of individuals and remains a leading cause of pain, mobility impairment, and disability in older adults. Epidemiological projections anticipate a rapid increase in OA incidence due to demographic transitions, including increased life expectancy, obesity prevalence, and sedentary habits. The socioeconomic burden is substantial, encompassing direct medical expenditures, loss of productivity, reduced quality of life, and long-term dependence on healthcare systems. In many low- and middle-income countries, inadequate access to specialized care further compounds the disability associated with OA, reinforcing the need for effective, accessible, and sustainable treatment modalities.[3][4]
1.2. Limitations of current therapeutic strategies
Contemporary management of OA relies predominantly on analgesics, NSAIDs, corticosteroid injections, and surgical interventions in advanced stages. While these modalities provide symptomatic relief, they do not effectively halt or reverse the underlying degenerative process. Long-term pharmacotherapy is frequently constrained by adverse effects such as gastrointestinal toxicity, renal impairment, and cardiovascular risks. Additionally DMOAD sremain limited in number, with most pharmacological agents offering only partial or temporary improvement. These shortcomings highlight the necessity for complementary strategies that target the disease at multiple biological levels.[5]
1.3. Rationale for integrative medicine
Integrative medicine offers a multidimensional framework that combines evidence-based traditional systems, such as Ayurveda, with advancements in modern pharmaceutical science. Ayurvedic formulations, bioactive phytocompounds, detoxification therapies, and lifestyle-based interventions provide multi-target actions, including anti-inflammatory, antioxidant, chondroprotective, and immunomodulatory effects. When synergistically aligned with pharmacological agents, physical therapy, and biomaterial innovations, integrative approaches have the potential to enhance efficacy, minimize side effects, and improve patient-centered outcomes. This holistic paradigm is particularly relevant for OA, where the pathology spans biomechanical, inflammatory, metabolic, and psychosocial domains.[6]
1.4. Scope and objectives of the review
This review aims to present a comprehensive analysis of osteoarthritis through the dual lens of Ayurveda and modern pharmacy. It synthesizes classical Ayurvedic concepts of Sandhigata Vata with contemporary mechanistic insights, evaluates evidence-based therapeutic interventions from both systems, and explores the potential for synergy in integrative practice. Additionally, the review outlines recent advances in drug delivery technologies, phytochemical characterization, and clinical research that support the development of robust integrative protocols. The overarching objective is to provide a cohesive scientific foundation for clinicians, researchers, and policymakers to advance integrative osteoarthritis management and promote collaborative translational research.[7]
2. Pathophysiology of Osteoarthritis
OA is a complex, multifactorial joint disorder characterized by progressive structural deterioration driven by biomechanical overload, inflammatory mediators, metabolic alterations, and age-related cellular senescence. Rather than being a purely “wear-and-tear” condition, current evidence positions OA as an active disease process involving coordinated dysfunction across cartilage, synovium, subchondral bone, and periarticular tissues. The following subsections summarize key pathogenic mechanisms that underpin contemporary understanding of OA.[8]
2.1. Articular cartilage degradation
Articular cartilage degradation represents a central hallmark of OA pathology. Chondrocyte homeostasis is disrupted by mechanical stress, inflammatory mediators, and metabolic imbalance, leading to reduced synthesis of type II collagen and aggrecan. Simultaneously, catabolic enzymes such as matrix metalloproteinases (MMP-1, MMP-3, MMP-13) and aggrecanases (ADAMTS-4, ADAMTS-5) accelerate extracellular matrix breakdown. The loss of proteoglycan content compromises cartilage elasticity and load-bearing capacity, rendering the tissue increasingly susceptible to fissuring, fibrillation, and eventual full-thickness erosion. As cartilage lacks intrinsic vascularity, its regenerative potential remains severely limited, perpetuating chronic degenerative change.[9]
2.2. Synovial inflammation and cytokine networks (IL-1β, TNF-α, IL-6)
Although traditionally considered non-inflammatory, OA is now recognized to involve low-grade, persistent synovitis. Synovial macrophages and fibroblast-like synoviocytes secrete potent cytokinesparticularly IL-1β, TNF-α, and IL-6that amplify joint inflammation and cartilage catabolism. IL-1β and TNF-α drive MMP expression, suppress chondrocyte anabolic pathways, and enhance nitric oxide and prostaglandin production. IL-6 modulates inflammatory signaling and contributes to osteoclastogenesis, worsening subchondral bone remodeling. This cytokine network creates a self-propagating loop that sustains tissue destruction and pain sensitization.[10]
2.3. Role of oxidative stress and reactive oxygen species (ROS)
Oxidative stress plays an increasingly acknowledged role in OA progression. Chondrocytes exposed to excessive ROSgenerated through mitochondrial dysfunction, inflammatory stimuli, and mechanical overloadundergo oxidative damage to lipids, proteins, and DNA. Elevated ROS levels impair autophagy, exacerbate cellular senescence, and trigger apoptosis. Moreover, ROS activate redox-sensitive transcription factors that promote catabolic gene expression. The cumulative effect is accelerated matrix breakdown and diminished reparative capacity.[11]
2.4. Subchondral bone changes and osteophyte formation
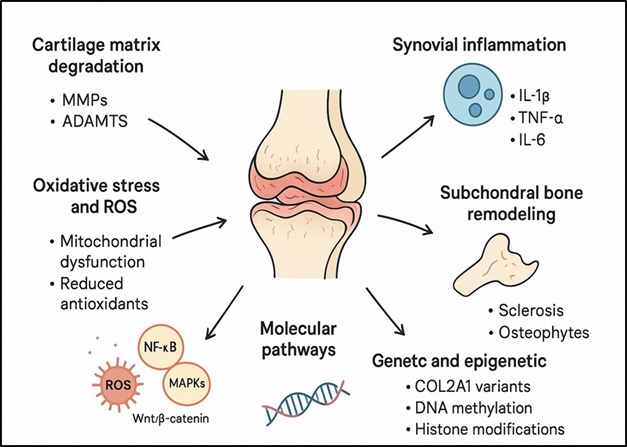
Subchondral bone undergoes profound structural alterations in OA. Early changes include increased bone turnover, microcrack formation, and sclerosis, leading to altered biomechanical stiffness at the cartilage–bone interface. Dysregulated osteoblast and osteoclast activity contributes to thickening of the subchondral plate and formation of fibrovascular channels. Osteophytesmarginal bone outgrowths induced by local mechanobiological signaling develop as an attempted reparative response but ultimately contribute to pain, limited mobility, and joint deformity. [Figure 1] represents overview of the pathophysiology of osteoarthritis.[12]
2.5. Molecular pathways: NF-κB, MAPKs, Wnt/β-catenin
Several intracellular pathways orchestrate catabolic and inflammatory processes in OA. NF-κB is a key transcriptional regulator activated by cytokines and mechanical stress, governing expression of MMPs, COX-2, and pro-inflammatory mediators. MAPK signaling (ERK, JNK, p38) further modulates the balance between anabolic and catabolic responses in chondrocytes. Dysregulation of the Wnt/β-catenin pathway contributes to aberrant bone formation, chondrocyte hypertrophy, and cartilage calcification. Crosstalk among these pathways creates a complex molecular network that perpetuates joint degeneration.[13] The [Table 1] provides key pathophysiological mechanisms involved in osteoarthritis.
|
Pathophysiological Component |
Key Features |
Primary Molecular/Cellular Mediators |
Relevance to Disease Progression |
|---|---|---|---|
|
Articular Cartilage Degradation |
Loss of ECM integrity; reduced proteoglycans; collagen breakdown |
MMP-1, MMP-3, MMP-13; ADAMTS-4, ADAMTS-5; diminished type II collagen synthesis |
Weakens load-bearing capacity, initiates fissures and erosion; irreversible structural damage |
|
Synovial Inflammation |
Low-grade, chronic synovitis; synoviocyte activation |
IL-1β, TNF-α, IL-6; PGE2; nitric oxide; activated macrophages |
Drives catabolic signaling, pain, and swelling; promotes further cartilage destruction |
|
Oxidative Stress & ROS |
Mitochondrial dysfunction; accumulation of oxidative damage |
ROS (superoxide, hydrogen peroxide); reduced antioxidant enzymes; NOX enzymes |
Induces chondrocyte apoptosis, senescence, and autophagy impairment; intensifies matrix breakdown |
|
Subchondral Bone Remodeling |
Sclerosis, microcracks, increased bone turnover; osteophyte formation |
RANK/RANKL/OPG system; TGF-β; BMPs |
Alters biomechanical properties; osteophytes cause stiffness, pain, and deformity |
|
Molecular Pathways |
Aberrant intracellular signaling; inflammatory gene upregulation |
NF- κB , MAPK (ERK, JNK, p38), Wnt /β-catenin |
Enhances MMP expression, inflammatory mediator release, chondrocyte hypertrophy, and cartilage calcification |
|
Genetic & Epigenetic Factors |
Heritable susceptibility; altered gene regulation |
COL2A1 variants; DNA methylation; histone modifications; microRNAs (miR- 140, miR-146a) |
Influences disease onset, progression speed, and tissue-specific responses |
2.6. Genetic and epigenetic influences
Genetic predisposition accounts for significant interindividual variation in OA susceptibility. Polymorphisms in genes related to collagen synthesis (COL2A1), inflammatory pathways, and matrix remodeling enzymes have been associated with elevated risk. Epigenetic mechanisms including DNA methylation, histone modifications, and non-coding RNAs further modulate chondrocyte phenotype and inflammatory responses. Age-related epigenetic drift and microRNA dysregulation (e.g., miR-140, miR-146a) impair cartilage homeostasis, facilitating OA onset and progression.[14][15]
3. Ayurvedic Perspective on Osteoarthritis
Ayurveda conceptualizes OA within the broader framework of Vata-vyadhi, wherein structural and functional disturbances arise due to the derangement of Vatadosha. Classical texts describe joint disorders under the entity SandhigataVata, which closely parallels the clinical phenotype of OA. This perspective provides a multidimensional understanding that integrates biomechanical degeneration, metabolic imbalance, and systemic functional decline. Unlike modern frameworks that emphasize local tissue pathology, Ayurveda interprets OA as an outcome of systemic doshaimbalance, impaired Agni (digestive/metabolic fire), and progressive depletion of structural body tissues (dhatus).[16]
3.1. Understanding sandhigata vata
SandhigataVata refers to the localization of aggravated Vata within joint spaces (sandhi), resulting in dryness, reduced lubrication, pain, and structural deterioration. Classical descriptors such as sandhishoola (joint pain), sandhishotha (swelling), and hantisandhigataha (restricted mobility) correspond to hallmark OA manifestations. The inherent properties of Vataruksha (dry), laghu (light), chala (mobile)mirror physiological processes such as cartilage dehydration, synovial fluid reduction, and instability within degenerating joints. This model emphasizes the role of systemic Vata dysregulation as the primary driver of local degenerative changes.[17]
3.2. Etiopathogenesis: Vata vruddhi, dhatukshaya, and ama formation
The Ayurvedic pathogenesis of SandhigataVata involves three interlinked mechanisms:
VataVruddhi (Vata aggravation): Triggered by aging, excessive physical strain, irregular diet, and stress, leading to enhanced catabolic activity. This manifests as breakdown of cartilage matrix and impaired joint lubrication. Dhatukshaya (tissue depletion): Progressive loss of Asthi (bone) and Majja (marrow) dhatus weakens structural support of joints. This aligns with contemporary concepts of cartilage loss, thinning subchondral bone, and reduction in proteoglycan content. Ama formation (toxic metabolic by-products): Impaired Agni produces ama, a pro-inflammatory, circulating toxin that obstructs microchannels (srotas) and promotes swelling and stiffness. This correlates with inflammatory mediators, oxidative stress markers, and synovial effusions observed in OA.Together, these processes create a pathological milieu conducive to chronic joint degeneration.[16][18]
3.3. Lakshanas (clinical symptoms) as defined in classics
Ayurvedic texts delineate distinctive symptoms of SandhigataVata, many of which exhibit strong parallels to OA phenotypes:
Shoola: Persistent, activity-linked joint pain. Stabdhata: Morning stiffness and reduced joint play. Shotha: Intermittent swelling due to ama accumulation. Prasarana-akunchanavedana: Pain on extension and flexion. Atopa: Crepitus-like sounds, resonating with cartilage wear. Kshayalakshanas: Wasting of periarticular tissues.
These classical lakshanas align closely with clinical criteria applied in rheumatology such as pain on movement, stiffness, crepitus, and restricted range of motion.[16][17][18][19]
3.4. Ayurvedic diagnostic considerations[20]
Ayurvedic diagnosis employs integrative assessment tools to evaluate systemic imbalance:
NadiPariksha (pulse diagnosis): Reveals Vata predominance and fluctuating rhythm patterns indicative of degenerative tendencies. JihvaPariksha (tongue examination): Coated tongue suggests ama presence, while cracks reflect chronic Vata elevation. Mala Pariksha: Hard, dry stools signal digestive hypo-function and Vata aggravation. Bala Assessment: Includes rogi-bala (patient vitality) and roga-bala (disease severity), guiding individualized therapy intensity.
These parameters enable holistic evaluation beyond localized joint changes, incorporating metabolic, digestive, and systemic factors.[21]
3.5. Comparative mapping of ayurvedic concepts to modern pathology
Ayurvedic constructs correlate strongly with contemporary scientific understanding of OA. The [Table 2] summarizes comparative mapping of ayurvedic concepts to modern pathology.
|
Ayurvedic Concept |
Modern Correlate |
|---|---|
|
VataVruddhi |
Catabolic dominance, neurogenic inflammation, decreased synovial fluid |
|
Dhatukshaya |
Cartilage loss, osteophyte formation, subchondral bone remodeling |
|
Ama accumulation |
Cytokine-mediated inflammation (IL-1β, TNF-α), oxidative stress |
|
Srotorodha ( microchannelobstruction ) |
Impaired microcirculation, synovial thickening |
|
Rukshata (dryness) |
Dehydrated cartilage matrix, reduced proteoglycans |
|
Sandhikshobha |
Mechanical wear, joint instability |
4. Current Pharmacotherapeutic Options in OA
Contemporary pharmacological management of OA primarily targets symptomatic control rather than structural reversal. Existing interventions focus on reducing nociception, dampening synovial inflammation, and improving joint function, yet no modality has demonstrated consistent disease-modifying potential in routine clinical practice. This section critically examines current drug classes, their mechanistic basis, therapeutic relevance, and inherent limitations.[23]
4.1. NSAIDs and analgesics
NSAIDs remain first-line agents for pharmacological management of OA due to their ability to inhibit cyclooxygenase isoenzymes (COX-1/COX-2), resulting in decreased prostaglandin synthesis and pain modulation. Both non-selective NSAIDs (ibuprofen, diclofenac, naproxen) and selective COX-2 inhibitors (celecoxib, etoricoxib) provide meaningful short-term analgesia and functional improvement. Paracetamol, though widely used, exhibits limited efficacy in moderate-to-severe OA and is no longer preferred as monotherapy. Despite clinical utility, chronic NSAID exposure is associated with gastrointestinal ulceration, renal impairment, hepatotoxicity, and increased cardiovascular risk, underscoring the need for safer long-term alternatives.[24]
4.2. Corticosteroids and intra-articular injections
Intra-articular corticosteroids (triamcinolone, methylpredniso- lone) offer rapid relief by suppressing synovial macrophage activation, cytokine release, and inflammatory infiltration. They are particularly useful during acute inflammatory flares. However, their benefits are transient, generally lasting 2–6 weeks, and repeated administration may accelerate cartilage degeneration by impairing chondrocyte metabolism. Systemic corticosteroids have minimal therapeutic rationale in OA due to unfavorable risk profiles. Alternative injectables such as local anesthetics or combination formulations are employed selectively but lack disease-modifying evidence.[25]
4.3. Viscosupplements (hyaluronic acid)
Viscosupplementation involves intra-articular administration of Hyaluronic Acid (HA), aiming to restore synovial fluid viscoelasticity, support lubrication, and modulate mechanotransduction pathways. High-molecular-weight and cross-linked HA preparations demonstrate variable but sometimes significant improvement in pain and joint mobility. Mechanistically, HA interacts with CD44 receptors, promoting anti-inflammatory and chondroprotective effects. However, clinical outcomes remain inconsistent across populations, and meta-analyses report marginal superiority over placebo. Cost variability, repeated injection requirements, and limited efficacy in advanced OA further restrict widespread adoption.[26][27]
4.4. DMOADs: Current status and limitations
DMOADs represent an aspirational class aimed at halting or reversing structural joint damage. Several investigational agents including glucosamine derivatives, chondroitin sulfate, sprifermin (FGF-18), and Wnt pathway modulatorshave demonstrated promising preclinical results. Nevertheless, their translation into definitive clinical benefit remains elusive. Challenges arise from OA’s heterogeneous pathogenesis, slow disease progression, and lack of sensitive biomarkers to track cartilage regeneration. To date, no DMOAD has gained regulatory approval, highlighting the urgent need for robust, longitudinal clinical data and improved mechanistic understanding.[28]
4.5. Biologicals (IL-1 inhibitors, TNF-α blockers)
Given the central role of inflammatory cytokines in OA pathobiology, biologics targeting IL-1 (anakinra, canakinumab) and TNF-α (etanercept, adalimumab) have been explored. These agents attenuate synovial inflammation and modulate catabolic enzyme activity. However, clinical trials in OA populations have shown limited improvements in pain or radiographic progression compared with their efficacy in rheumatoid arthritis. High cost, immunosuppression risks, and logistical challenges of parenteral administration have impeded their acceptance in standard OA care.[29]
4.6. Safety issues, adverse drug reactions, and unmet clinical needs
Despite therapeutic advances, current pharmacological approaches are constrained by safety liabilities and insufficient long-term efficacy. NSAIDs pose gastrointestinal, renal, and cardiovascular hazards; corticosteroid injections risk cartilage atrophy; HA injections may induce transient synovitis; and biologics carry substantial infection risks. The lack of reliable DMOADs remains a critical gap, leaving clinicians reliant on symptomatic treatments that do not halt disease progression. Moreover, inter-individual variability in drug response, polypharmacy in older adults, and increasing emphasis on personalized and minimally invasive care demand integrative strategies that deliver sustained pain relief while minimizing systemic toxicity.[30]
5. Evidence-Based Ayurvedic Therapeutics
5.1. Internal medications
Ayurvedic internal medications play a pivotal role in mitigating the underlying Vata imbalance and tissue degeneration characteristic of SandhigataVata. Guggulu-based formulations including Yograj Guggulu, Mahayograj Guggulu, and Trayodashang Gugguluare widely utilized owing to their multi-target pharmacodynamic profile. These formulations exhibit potent anti-inflammatory, antioxidant, and anti-nociceptive properties attributed to guggulsterones and volatile constituents that modulate NF-κB signaling, reduce prostaglandin synthesis, and enhance microcirculation within joint tissues. In addition, Shallaki (Boswelliaserrata) offers significant chondroprotective activity, primarily through boswellic acids which inhibit 5-lipoxygenase pathways and attenuate leukotriene-mediated cartilage degradation. Herbal agents such as Ashwagandha (Withaniasomnifera), Nirgundi (Vitexnegundo), Shunthi (Zingiber officinale), and Rasna (Pluchealanceolata) contribute synergistically by reducing oxidative stress, modulating cytokine release, and supporting neuromuscular stability. Rasayana and Vata-shamaka herbs restore tissue resilience, counteract dhatukshaya, and support metabolic homeostasis, thereby promoting long-term joint health.[18][31]
5.2. External therapies
External therapies form an essential component of Ayurvedic OA management by improving local circulation, reducing stiffness, and enhancing joint lubrication. Abhyanga (therapeutic oil massage) employs medicated oils such as Mahanarayana or Ksheerabala to modulate neuromuscular tone and alleviate pain. JanuBasti and Kati Basti, in which warm medicated oil is retained over target joints, provide sustained thermal and pharmacological effects that ease synovial stiffness and improve functional mobility.[32] Sweating procedures such as PatraPindaSweda (bolus fomentation with herbal leaves) and NadiSweda (steam fomentation) facilitate vasodilation, reduce local edema, and enhance synovial diffusion. These treatments collectively improve joint biomechanics and complement internal medications by enhancing tissue receptivity.[33]
5.3. Panchakarma interventions
Panchakarma therapies offer deeper detoxification and systemic correction of Vata derangements. Virechana (therapeutic purgation) reduces inflammatory mediators, improves hepatic metabolism, and helps eliminate ama, which is implicated in chronic inflammation. Basti Chikitsa, particularly Ksheera Basti and Matra Basti, is considered the cornerstone therapy for osteoarthritis due to its direct effect on Vata regulation. The medicated enemas deliver lipid-based formulations rich in nourishing and anti-inflammatory constituents, positively influencing neuromuscular control, colon health, and systemic Vata balance.[34]
5.4. Nutritional and lifestyle interventions (Āhāra–Vihāra)
Ayurveda emphasizes diet and lifestyle as foundational components of OA management. A Vata-pacifying dietwarm, unctuous, easily digestible foods enriched with spices such as ginger, turmeric, and garlichelps reduce systemic dryness and inflammation. Adequate protein sources, whole grains, and omega-rich dietary components support cartilage integrity. Lifestyle measures include regular low-impact exercises, controlled physical activity, adequate sleep, and avoidance of cold exposure or excessive strain on weight-bearing joints. Mind–body practices such as yoga and pranayama enhance flexibility, reduce stress-induced inflammation, and promote overall musculoskeletal stability.[35]
5.5. Clinical evidence supporting ayurvedic treatment
An increasing body of clinical research demonstrates the therapeutic potential of Ayurvedic interventions in osteoarthritis. Randomized controlled trials have reported significant improvements in pain scores, joint stiffness, and functional parameters following Guggulu-based formulations and Boswellia extracts. Panchakarma procedures particularly Basti—have shown superior outcomes in WOMAC and VAS scores, reflecting improved mobility and reduced dependence on NSAIDs. External therapies, when integrated with internal medications, have demonstrated enhanced efficacy through multimodal action supporting both symptomatic and structural improvements. Collectively, the clinical evidence highlights Ayurveda as a valid complementary system capable of addressing both symptomatic and pathophysiological components of osteoarthritis.[36]
6. Synergistic Potential
Integrating Ayurvedic therapeutics with contemporary pharmaceutical interventions presents a scientifically compelling strategy for addressing the complex, multifactorial pathogenesis of OA. While modern pharmacology primarily emphasizes targeted molecular inhibition, Ayurvedic medicine employs a holistic, systems-based approach that modulates multiple interconnected biological pathways. This convergence offers a unique opportunity to combine rapid symptom relief with long-term disease-modifying effects, forming a comprehensive and patient-centric therapeutic paradigm.[37]
6.1. Conceptual synergy
Modern OA pharmacotherapy, including NSAIDs, corticosteroids, and biologics, typically relies on specific molecular targets such as COX enzymes, pro-inflammatory cytokines, or receptor-mediated pathways. Although highly effective in symptom suppression, these agents often fail to modify the structural progression of OA and may result in systemic adverse events. In contrast, Ayurvedic botanicals (e.g., Boswelliaserrata, Commiphorawightii, Withaniasomnifera) exhibit multi-target actions. Their phytoconstituents simultaneously influence inflammatory cascades, oxidative stress markers, nociceptive signaling, extracellular matrix turnover, and immune modulation. This multi-layered pharmacodynamic activity aligns with the polygenic and heterogeneous nature of OA. When integrated, the targeted precision of modern drugs can complement the broad-spectrum regulatory effects of Ayurvedic formulations, forming a rational therapeutic synergy.[38][39]
6.2. Anti-inflammatory, antioxidant & chondroprotective convergence
The pathobiology of OA is driven by chronic low-grade inflammation, ROS-induced cellular injury, and progressive cartilage degradation. Ayurvedic herbs rich in boswellic acids, guggulsterones, curcuminoids, and withanolides exhibit potent downregulation of NF-κB, COX-2, LOX-5, and MAPK pathways. Concurrently, modern pharmaceuticals offer rapid suppression of prostaglandin synthesis and cytokine signaling. When combined, these approaches amplify anti-inflammatory efficacy, reinforce endogenous antioxidant defenses, and enhance chondroprotection. Polyphenolic compounds from Ayurvedic drugs help stabilize chondrocyte metabolism, inhibit Matrix Metalloproteinases (MMPs), and promote proteoglycan synthesis—effects that modern analgesics alone cannot achieve.[40]
6.3. Complementary benefits: Enhanced efficacy with fewer adverse effects
Integrative regimens have the potential to lower the dosage requirements of NSAIDs or corticosteroids due to the additive anti-inflammatory effects of herbal agents. Reduced dosage directly correlates with decreased incidence of gastrointestinal, renal, and cardiovascular adverse effects. Meanwhile, Ayurvedic interventions such as Rasayana therapy support systemic resilience, improve gut integrity, and modulate metabolic processes, thereby enhancing overall therapeutic tolerance. This complementary benefitpotentiation of efficacy alongside mitigation of toxicityrepresents a key advantage of integrative OA management.[41]
6.4. Herb–drug interactions
The co-administration of herbal and modern drugs necessitates careful evaluation of pharmacokinetic and pharmacodynamic interactions. Beneficial interactions include improved drug absorption (e.g., piperine enhancing bioavailability of curcuminoids), synergistic suppression of inflammatory mediators, and stabilization of drug-induced oxidative stress.However, harmful interactions can arise from CYP450 modulation, P-glycoprotein interference, or competitive receptor binding. For instance, excessive guggulsterone may influence thyroid hormone metabolism, while curcumin can potentially alter anticoagulant activity. Thus, integrative practice requires rigorous assessment of dose, timing, and patient-specific factors.[42][43]
6.5. Evidence from integrative clinical models
Emerging clinical studies report that combining herbal formulations with standard OA pharmacotherapy improves pain scores, gait parameters, and functional outcomes more significantly than monotherapy. Trials integrating Boswellia, Guggulu, and Ashwagandha with NSAIDs have shown reduced VAS and WOMAC scores, enhanced joint mobility, and improved inflammatory biomarkers. Panchakarma-based interventions, when used as adjunctive therapy, demonstrate superior long-term symptom control and reduced relapse rates. These findings underscore the translational value of integrative models, validating the mechanistic synergy between Ayurveda and modern pharmacy and reinforcing the need for larger, well-designed clinical trials.[44]
7. Phytochemistry and Mechanisms of Key Ayurvedic Herbs
The therapeutic relevance of Ayurvedic botanicals in OA is strongly supported by their diverse phytochemical profiles, which confer multi-targeted modulation of inflammatory, oxidative, and degenerative pathways. Unlike single-molecule pharmaceutical agents, these herbs contain complex matrices of bioactive constituents capable of interacting with multiple signaling networks that underlie OA pathophysiology. Their mechanistic versatility positions them as promising adjuncts to contemporary pharmacotherapeutics, especially in chronic, low-grade inflammatory disorders such as OA.[45]
7.1. Boswellic acids and 5-LOX inhibition
Boswellia serrata resin is rich in pentacyclic triterpenoids collectively known as boswellic acids (BAs), of which acetyl-11-keto-β-boswellic acid (AKBA) is the most pharmacologically potent. AKBA selectively inhibits 5-lipoxygenase (5-LOX), thereby reducing leukotriene synthesis—a critical driver of synovial inflammation and cartilage catabolism. In addition to 5-LOX blockade, BAs modulate NF-κB activation, downregulate matrix metalloproteinases (MMP-3, MMP-13), and attenuate chondrocyte apoptosis. Their dual anti-inflammatory and chondroprotective properties contribute to improved joint function and reduced pain scores in clinical studies.[46]
7.2. Guggulsterones and anti-inflammatory pathways
Commiphora mukul contains guggulsterones (E- and Z-isomers), steroid-like phytoconstituents known for broad immunomodulatory effects. Guggulsterones antagonize the farnesoid X receptor (FXR), leading to downstream suppression of inflammatory gene expression. They inhibit TNF-α, IL-1β, and COX-2 signaling, and reduce nitric oxide production by downregulating inducible Nitric Oxide Synthase (iNOS). Guggulsterones also interfere with NF-κB nuclear translocation, thereby reducing expression of catabolic mediators that accelerate cartilage breakdown. Their lipid-modulating properties indirectly benefit OA patients by reducing metabolic stressors associated with joint inflammation.[47]
7.3. Withanolides from ashwagandha
Withania somnifera roots contain withanolides steroidal lactones structurally analogous to adaptogenic and anti-inflammatory compounds. Withaferin A and Withanolide D are key molecules associated with immunoregulatory activity. Withanolides inhibit the JAK-STAT and NF-κB pathways, suppress pro-inflammatory cytokine production, and protect chondrocytes from oxidative injury. Their antioxidant activity reduces ROS-mediated cartilage degradation, while their anti-hyperalgesic effects help mitigate chronic pain. Additionally, withanolides stabilize mitochondrial membranes and promote cellular resilience, supporting long-term cartilage health.
7.4. Flavonoids, terpenoids, and alkaloids in OA modulation.[48]
Many Ayurvedic herbs including Rasna (Pluchea lanceolata), Nirgundi (Vitexnegundo), Shunthi (Zingiber officinale), and Eranda (Ricinus communis) derive their anti-osteoarthritic activities from flavonoids (quercetin, luteolin), terpenoids (cineole, limonene), and alkaloids (casticine). These compounds exert synergistic effects by scavenging reactive oxygen species, stabilizing collagen architecture, and reducing prostaglandin and leukotriene synthesis. Flavonoids inhibit MMPs and ADAMTS enzymes responsible for aggrecan degradation; terpenoids modulate nociceptive pathways, and certain alkaloids exhibit selective COX-2 suppression. The combined modulation of inflammatory mediators and structural proteins enhances joint lubrication, elasticity, and resilience.[49]
7.5. Preclinical and molecular docking insights
Preclinical investigations reveal that major Ayurvedic phytoconstituents demonstrate strong affinity for molecular targets implicated in OA progression. Molecular docking studies show AKBA binding tightly within the 5-LOX active pocket, while guggulsterones display favorable interactions with NF-κB regulators and COX-2 catalytic sites. Withanolides exhibit high docking scores with JAK kinases, caspase-3, and MMP-13, supporting their inhibitory potential. In vivo models consistently demonstrate reduction of paw edema, cartilage erosion, and serum inflammatory markers following treatment with these phytochemicals. Emerging systems-biology approaches further highlight their poly-pharmacological nature, suggesting cumulative effects on chondrocyte survival pathways, synovial homeostasis, and extracellular matrix preservation.[50]
8. Discussion
8.1. Advances in modern drug delivery and ayurvedic integration
Recent progress in pharmaceutical technology has opened new avenues for enhancing the efficacy of both conventional OA therapeutics and Ayurvedic phyto-interventions. Modern drug delivery systems enable improved bioavailability, targeted action, and sustained therapeutic outcomes—attributes particularly relevant in chronic degenerative conditions such as OA. When combined with time-tested Ayurvedic formulations, these innovations offer a promising integrative platform to optimize clinical benefits while minimizing systemic toxicities.[51][52]
8.2. Nanotechnology-enabled drug delivery
Nanotechnology has revolutionized musculoskeletal therapeutics by enabling site-specific delivery of active molecules to inflamed synovium and degenerated cartilage. Liposomes, solid lipid nanoparticles (SLNs), polymeric nanoparticles, and nanomicelles enhance membrane penetration, prolong circulation half-life, and improve solubility of hydrophobic drugs commonly used in OA management. For herbal medicine, nanocarriers can overcome challenges such as poor aqueous solubility, rapid metabolism, and low intestinal absorption. Phytoconstituents like boswellic acids, guggulsterones, and withanolides have been successfully formulated into nanoparticle systems, demonstrating improved anti-inflammatory and chondroprotective activity in preclinical models. Moreover, nanoparticle-mediated targeting of the NF-κB and COX-2 pathways holds particular relevance in modulating OA-related biochemical cascades.[53]
8.3. Encapsulation of herbal phytoconstituents
Encapsulation technologies such as nanoemulsions, phytosomes, polymeric nanocapsules, and lipospheres provide structural protection to fragile phytochemicals while regulating their release kinetics. Encapsulation enhances oral stability, shields bioactive components from gastrointestinal degradation, and ensures controlled diffusion into systemic circulation.For Ayurvedic interventions, the encapsulation of bioactive moieties from herbs such as Boswellia, Curcuma longa, Terminalia chebula, and Withania somnifera offers a mechanistic advantage by facilitating targeted accumulation in joint tissues. These systems also reduce dose variability and batch-to-batch inconsistencya persistent challenge in herbal therapeutics.[54]
8.4. Transdermal and topical novel systems
Transdermal Drug Delivery Systems (TDDS) provide a non-invasive route for sustained release of anti-arthritic agents directly at the site of inflammation, thereby reducing gastrointestinal and renal adverse effects associated with systemic NSAID therapy. Novel delivery matrices such as microemulsion gels, nano-structured lipid carriers, and polymer-based patches exhibit enhanced skin permeation and prolonged therapeutic retention.Integrating Ayurvedic external therapies with advanced transdermal platforms offers additional potential. Herbal extracts traditionally administered via Abhyanga or Lepa can be incorporated into nano-gel or hydrogel-based carriers to improve dermal absorption and provide localized chondroprotective, analgesic, and anti-inflammatory effects.[55]
8.5. Controlled release formulations for chronic OA
Controlled release systems are particularly relevant for long-term OA management where continuous suppression of inflammation and pain is required. Hydrophilic matrix tablets, osmotic pumps, biodegradable implants, and microsphere systems can provide steady-state plasma levels, enhance therapeutic compliance, and reduce dosing frequency. When applied to herbal interventions, controlled release formulations help maintain consistent concentrations of phytochemicals, aligning modern pharmacokinetics with traditional Ayurvedic principles of sustained physiological balance (dhatuposhana). Long-acting formulations of curcuminoids, boswellic acids, and flavonoid-rich extracts have shown promise in extending anti-inflammatory effects with reduced dosing burden.[56]
8.6. Combining modern delivery with ayurvedic herbal extracts
The convergence of pharmaceutical technology with Ayurveda enables the development of hybrid therapeutics that leverage the strengths of both systems. Polyherbal extracts can be incorporated into nanocarriers, transdermal matrices, or controlled release systems to produce optimized integrative formulations with enhanced therapeutic precision.[57] Such hybrid approaches allow multi-target engagementmodulating inflammatory mediators, protecting chondrocytes, and promoting extracellular matrix restorationwhile ensuring pharmacokinetic standardization. Furthermore, integrating Ayurvedic herbs with modern delivery systems provides opportunities for developing DMOAD-like phytopharmaceuticals. These advancements highlight a transformative paradigm for OA management, wherein modern drug delivery technologies enhance the bioefficacy, safety, and clinical relevance of Ayurvedic therapeutics, fostering a truly integrative approach for chronic joint disorders.[58]
9. Challenges in Integrative Osteoarthritis Management
9.1. Standardization of herbal raw materials
A major challenge in integrating Ayurveda with modern pharmacy is the inherent variability in herbal raw materials. Phytochemical composition of medicinal plants fluctuates depending on agroclimatic conditions, soil quality, harvesting season, plant maturity, and post-harvest handling. These variations influence the concentration of active constituents such as boswellic acids, guggulsterones, and withanolides, ultimately affecting therapeutic consistency. The absence of universally accepted monographs for several classical herbs further complicates standardization. Establishing robust, validated methods for raw material authentication—using chromatographic fingerprints, DNA barcoding, and advanced spectroscopic toolsis essential for ensuring batch-to-batch uniformity in integrative osteoarthritis formulations.[29]
9.2. Quality control and GMP compliance
Quality assurance in integrative products requires adherence to stringent Good Manufacturing Practices (GMP). Ayurvedic preparations, when combined with modern formulations, must meet pharmaceutical-grade specifications related to purity, potency, microbial limits, heavy metal content, and residual solvents. Ensuring contamination-free, reproducible products demands modern analytical techniques such as HPTLC, LC–MS/MS, and ICP-MS. However, many small-scale Ayurveda manufacturers face infrastructural and technical limitations in implementing advanced QC systems. Harmonization of GMP guidelines across AYUSH and modern pharmaceutical sectors is crucial for ensuring the reliability of integrative therapeutics.[23]
9.3. Dose optimization and safety monitoring
Determining optimal dose ranges for herbal formulations remains a key scientific gap. Unlike single-molecule pharmaceuticals, Ayurvedic multi-component preparations exhibit complex pharmacokinetics influenced by synergistic or antagonistic interactions among constituents. Establishing accurate dose–response relationships requires well-designed pharmacokinetic/pharmacodynamic (PK/PD) studies, which are currently limited. Safety monitoring is equally important, as herb–drug interactions may potentiate or attenuate the activity of NSAIDs, corticosteroids, or DMOADs commonly used in osteoarthritis. Integrating pharmacovigilance mechanisms and real-world data reporting will strengthen risk assessment in integrative care.[59]
9.4. Regulatory challenges
India’s dual regulatory frameworkAYUSH for traditional medicines and CDSCO for modern pharmaceuticalsposes complexities for integrative product approval. Variations in documentation requirements, clinical trial norms, labeling standards, and claims validation create barriers to developing combined regimens. The absence of a dedicated regulatory category for “integrative therapeutics” results in ambiguity around classification, marketing authorization, and post-market surveillance. Clear, harmonized guidelines that define permissible combinations, safety testing protocols, and evidence thresholds are urgently needed to streamline innovation in integrative osteoarthritis management.[60]
9.5. Patient-centered barriers: Acceptability and adherence
Patient perceptions strongly influence adherence to integrative regimens. Differences in dosage forms, treatment durations, taste, or complexity of Ayurvedic therapies may reduce compliance, particularly in elderly OA patients. Misconceptions regarding the safety of herbal drugs or the perceived slowness of Ayurvedic interventions can further hinder acceptance. Additionally, socio-economic factors, cultural preferences, and accessibility of trained integrative practitioners influence sustained engagement. Enhancing patient education, simplifying therapeutic protocols, and improving communication between Ayurvedic and allopathic practitioners are essential to overcoming these barriers.[61]
10. Research Gaps and Future Directions
10.1. Need for robust randomized controlled trials (RCTs) on integrative OA protocols
Current clinical evidence for Ayurvedic and integrative OA interventions is promising but limited by methodological heterogeneity, small sample sizes, inadequate blinding, non-standardized formulations, and inconsistent outcome reporting. Large, multicentric, and rigorously designed RCTs are urgently required to validate integrative treatment algorithms that combine herbal formulations, Panchakarma procedures, and modern pharmacotherapies. Standardized protocols including dose uniformity, biomarker-based patient stratification, and validated endpoints (e.g., WOMAC, VAS, joint function indices)are necessary to generate reproducible and generalizable evidence. Incorporating comparator arms with standard-of-care medicines will help evaluate additive or synergistic benefits while clarifying safety profiles and herb–drug interaction risks.[62]
10.2. Omics-based profiling of ayurvedic herbs
Ayurvedic botanicals exhibit complex phytochemical matrices with multi-target therapeutic potential. However, their molecular signatures and bioactive networks remain underexplored. Integrating genomics, transcriptomics, proteomics, metabolomics, and phytomics can elucidate the mechanistic pathways through which herbs such as Boswellia serrata, Commiphora wightii, and Withania somnifera exert chondroprotective, anti-inflammatory, and immunomodulatory effects. Multi-omics profiling can also support quality control, chemotype identification, authentication, and batch-to-batch consistency. Such datasets will enable the development of phytochemical fingerprints and predictive biomarkers for therapeutic responsiveness, improving standardization and clinical reliability.[63]
10.3. Systems biology approach for multi-target therapy
The multi-factorial nature of OAcharacterized by intertwined inflammatory, metabolic, oxidative, and biomechanical pathwaysnecessitates a systems-level therapeutic strategy. Ayurvedic formulations, due to their polyherbal composition, inherently operate through network-level modulation rather than single-target inhibition. Applying systems biology tools, including computational pathway modeling, network pharmacology, and molecular docking, can illuminate herb–compound–target interactions and identify synergistic molecular clusters. This approach may guide the rational design of integrative formulations that optimize efficacy by simultaneously modulating cytokine signaling, extracellular matrix turnover, chondrocyte survival, and oxidative stress pathways.[64]
10.4. Digital therapeutics and AI for personalized disease management
Digital platforms represent an emerging frontier in OA care. Artificial Intelligence (AI), Lachine Learning (ML), and digital therapeutics offer opportunities to personalize integrative treatment plans based on patient-specific phenotypes, lifestyle patterns, mobility data, and real-time symptom monitoring. AI-assisted algorithms can stratify patients into subtypes aligned with Ayurvedic Prakriti classifications and modern clinical biomarkers, enabling tailored interventions. Wearable sensors and mobile health applications can continuously track gait dynamics, pain fluctuations, range of motion, and treatment adherence. Integrating these data streams can support predictive analytics for disease progression and facilitate dynamic adjustment of integrative therapeutics.[65]
10.5. Bridging traditional knowledge with pharmacological sciences
A critical gap in integrative OA management lies in harmonizing the epistemological frameworks of Ayurveda and modern pharmacology. Bridging this divide requires structured efforts to reinterpret classical Ayurvedic conceptssuch as SandhigataVata, Rasayana, and Agnithrough biochemical, molecular, and physiological correlates. Collaborative research platforms should promote cross-disciplinary training, shared databases, and jointly developed experimental methodologies. Advances in pharmacognosy, molecular pharmacology, and biopharmaceutics can facilitate the translation of traditional formulations into standardized, evidence-based products. Regulatory convergence between AYUSH and contemporary drug development frameworks is equally important to streamline approval pathways, ensure safety, and encourage innovation.[66]
11. Conclusion
OA remains a complex, multifactorial disorder with limited long-term efficacy of conventional pharmacotherapy. Integrative approaches that combine Ayurvedic principles with modern pharmaceutical interventions offer a unique paradigm to address both symptomatic relief and disease-modifying outcomes. Ayurveda, with its holistic focus on systemic balance, anti-inflammatory herbs, detoxification procedures, and lifestyle modifications, provides a multi-targeted framework that complements the precision and mechanistic specificity of modern pharmacology. This synergy enables not only attenuation of inflammation and pain but also potential enhancement of cartilage preservation, improved joint function, and reduction of adverse effects commonly associated with long-term use of NSAIDs and corticosteroids.The integration of standardized herbal formulations, Panchakarma therapies, and dietary regimens with evidence-based modern drugs represents a patient-centered approach that acknowledges the heterogeneity of OA pathophysiology. Clinical and preclinical evidence suggests that phytoconstituents such as boswellic acids, guggulsterones, and withanolides can exert chondroprotective, anti-oxidative, and immunomodulatory effects, which may enhance the efficacy of contemporary pharmaco therapeutics when used judiciously. Despite promising outcomes, the full potential of integrative OA management remains underexplored due to the lack of systematic clinical trials and mechanistic studies bridging traditional knowledge with modern science. Collaborative research initiatives between Ayurveda and modern pharmacy are essential to establish standardized protocols, optimize dosing strategies, and validate therapeutic endpoints. Such interdisciplinary efforts could ultimately lead to safer, more effective, and personalized OA interventions, fostering translational frameworks that integrate ancient wisdom with contemporary biomedical innovation. The convergence of these disciplines holds significant promise for advancing osteoarthritis management in a scientifically rigorous, holistic, and patient-centric manner.
12. Source of Funding
None.
13. Conflict of Interest
None.
References
- Loeser R, Goldring S, Scanzello C, Goldring M. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012;64(6):1697-707. [Google Scholar] [Crossref]
- Coaccioli S, Sarzi-Puttini P, Zis P, Rinonapoli G, Varrassi G. Osteoarthritis: New Insight on Its Pathophysiology. J Clin Med. 2022;11(20). [Google Scholar] [Crossref]
- Han X, Zhang C, Guan B, Zhou H, Kong X, Feng S. Burden of osteoarthritis in older adults (aged ≥55 years) in the United States and China: a comparative analysis of temporal trends, risk factor contributions, and projected burden to 2030 using global burden of disease study 2021 data. Front Med (Lausanne). 2030;12. [Google Scholar] [Crossref]
- Ma W, Chen H, Yuan Q, Chen X, Li H. Global, regional, and national epidemiology of osteoarthritis in working-age individuals: insights from the global burden of disease study 1990–2021. Sci Rep. 2025;15(1). [Google Scholar] [Crossref]
- Del Río E. Pharmacist-Driven Chondroprotection in Osteoarthritis: A Multifaceted Approach Using Patient Education, Information Visualization, and Lifestyle Integration. . Pharmacy (Basel). 2025;13(4). [Google Scholar] [Crossref]
- Jha S, Singh N, Shanker O, Antil I, Baghel J, Huddar V e. Integrative Approaches in Oncology: Bridging Ayurvedic Medicine and Modern Therapeutics. Front Nat Prod. 2025. [Google Scholar] [Crossref]
- Patil S, Rangnekar S. A Review on Ayurvedic Management of Sandhivata with Respect to Osteoarthritis. World J Adv Res Rev. 2022;16(2):1032-1036. [Google Scholar] [Crossref]
- Yunus M, Nordin A, Kamal H. Pathophysiological Perspective of Osteoarthritis. Medicina (Kaunas). 2020;56(11). [Google Scholar] [Crossref]
- Ashruf O, Ansari M. Natural Compounds for Cartilage Matrix Protection in Osteoarthritis. Life. 2023;13(1). [Google Scholar] [Crossref]
- Peng R, Lin Q, Yang Z, Li H, Li J, Xing D. Fibroblast-Myofibroblast Transition in Osteoarthritis Progression: Current Insights. Int J Mol Sci. 2025;26(16). [Google Scholar] [Crossref]
- Floramo J, Molchanov V, Liu H, Liu Y, Craig S, Yang T. Stressors as Causative Agents in OA Pathogenesis. Biomolecules. 2023;13(5). [Google Scholar] [Crossref]
- Goldring S. Alterations in periarticular bone and cross talk between subchondral bone and articular cartilage in osteoarthritis. Ther Adv Musculoskelet Dis. 2012;4(4):249-58. [Google Scholar] [Crossref]
- Guo Q, Jin Y, Chen X, Ye X, Shen X, Lin M. NF-κB in Biology and Targeted Therapy. Signal Transduct Target Ther. 2024;9(1). [Google Scholar] [Crossref]
- Aubourg G, Rice S, Bruce-Wootton P, Loughlin J. Genetics of osteoarthritis. Osteoarthritis Cartilage. 2022;30(5):636-649. [Google Scholar] [Crossref]
- Kiełbowski K, Herian M, Bakinowska E, Banach B ST, Pawlik A. The Role of Genetics and Epigenetic Regulation in the Pathogenesis of Osteoarthritis. Int J Mol Sci. 2023;24(14). [Google Scholar] [Crossref]
- Meghashree, Shet B, Kalkura K. Unravelling SandhigataVata (Osteoarthritis). J Ayurveda Integr Med Sci. 2025;10(1):196-202. [Google Scholar] [Crossref]
- Singh B, Bansal J, Kumar A, Singh N, Kumar P. Sandhigatavata and Osteoarthritis: A Review. Ayushdhara. 2023. [Google Scholar] [Crossref]
- Akhtar B, Mahto R, Dave A, Shukla V. Clinical study on Sandhigata Vata w.s.r. to Osteoarthritis and its management by Panchatikta Ghrita Guggulu. Ayu. 2010;31(1):53-7. [Google Scholar] [Crossref]
- Sawarkar G, Sawarkar P. Prevention and Management of Osteoarthritis. Int J Res Ayurveda Pharm. 2013;4(3):454-458. [Google Scholar] [Crossref]
- Kumar P, Deshpande S, Nagendra H. Traditional practices and recent advances in Nadi Pariksha: A comprehensive review. J Ayurveda Integr Med. 2019;10(4):308-15. [Google Scholar] [Crossref]
- Tiwari Y, Dhakad H. NadiPariksha: An Ancient Ayurvedic Method. J Ayu Int Med Sci. 2022. [Google Scholar]
- Ingale D, Kulkarni P, Koppikar S, Harsulkar A, Moghe A, Jagtap S. Anti-Osteoarthritis Activity of Polyherbal Formulations. Indian J Pharmacol. 2018;50(1). [Google Scholar] [Crossref]
- Farinelli L, Riccio M, Gigante A, De Francesco F. Pain Management Strategies in Osteoarthritis. Biomedicines. 2024;12(4). [Google Scholar] [Crossref]
- Magni A, Agostoni P, Bonezzi C, Massazza G MP, Savarino V. Management of Osteoarthritis: Expert Opinion on NSAIDs. Pain Ther. 2021;10(2):783-808. [Google Scholar] [Crossref]
- Singer B, Chaimovitz D, Bucek T, Dayon E, Abbott-Korumi A, Spatz M. Corticosteroid Use in Musculoskeletal and Neuraxial Interventions: Effects on Glycemic Control. Medicina (Kaunas). 2025;61(5). [Google Scholar] [Crossref]
- Glinkowski W, Tomaszewski W. Intra-Articular Hyaluronic Acid for Knee OA. J Clin Med. 2025. [Google Scholar] [Crossref]
- Abate M, Pulcini D, Di Iorio A, Schiavone C. Viscosupplementation in Elderly OA. Curr Pharm Des. 2010. [Google Scholar] [Crossref]
- Brandt M, Malone J, Kean T. Advances and Challenges in the Pursuit of Disease-Modifying Osteoarthritis Drugs: A Review of 2010-2024 Clinical Trials. Biomedicines. 2025;13(2). [Google Scholar] [Crossref]
- Wang K, Luo H, Liu L, Gao H, Song Y, Li D. Blockade of IL-1 family cytokines in the treatment of rheumatoid arthritis. Front Pharmacol. 2025;16. [Google Scholar] [Crossref]
- Tummala S, Parmar R, Holle A, Brinkman J, Hassebrock J, Tokish J. Long-term nonsteroidal anti-inflammatory drug use is associated with rotator cuff tears in adult patients. JSES Int. 2025;9(3):666-71. [Google Scholar] [Crossref]
- Bora M, Sinha B, Dixi A, Jamadagni S, Gaidhani S, Gautam M. Anti-Arthritic Activity of Trayodashangguggulu, a Classical Ayurvedic Formulation, against Complete Freund’s Adjuvant-Induced Rheumatoid Arthritis in Rats. J Basic Appl Zool. 2024. [Google Scholar] [Crossref]
- Roshy J, Cherian A, Joseph C. Role of Abhyanga (Oil Massage) to Lead a Healthy Life. J Ayurveda. 2012. [Google Scholar]
- Bhusal N, Prakash S, Mangal G, Scholar P. Review on Patra Pinda Sweda: A Peculiar Ayurveda Bolus Fomentation. Int J Ayurveda Med. 2017. [Google Scholar]
- Suman M, Pradeep K, Panchakarma PfaHLTCBPaH. J Ayu Int Med Sci. J Ayu Int Med Sci. 2023. [Google Scholar]
- Payyappallimana U, Venkatasubramanian P. Exploring Ayurvedic Knowledge on Food and Health for Providing Innovative Solutions to Contemporary Healthcare. Front Public Health. 2016;4. [Google Scholar] [Crossref]
- Kachare K, Makhija D, Sharma A S, Srikanth N, Sharma B. Evaluation of Yograj Guggulu, Ashwagandha Churna and Narayana Taila in management of Osteoarthritis Knee: A study in tribal dominant community. J Ayurveda Integr Med. 2025;16(2). [Google Scholar] [Crossref]
- Sandeep C, Gupta V, Deshmukh V, Sardeshmukh S. Integrating Ayurvedic philosophy with modern technologies for drug research and development: A critical need of mechanistic insights for wider acceptability. J Ayurveda Integr Med. 2024;15(5). [Google Scholar] [Crossref]
- Jameel N, Dwivedi A, Khushtar M, Haider M, Nematullah M, Rahman M. Inflammation Demystified: An In-Depth Comprehensive Review. Biomed Res Ther. 2025. [Google Scholar] [Crossref]
- Ben Mrid R, Bouchmaa N, Ainani H, El Fatimy R, Malka G, Mazini L. Anti-rheumatoid drugs advancements: New insights into the molecular treatment of rheumatoid arthritis. Biomed Pharmacother. 2022;151. [Google Scholar] [Crossref]
- Nirmal P, Jagtap S, Narkhede A, Nagarkar B, Harsulkar A. New herbal composition (OA-F2) protects cartilage degeneration in a rat model of collagenase induced osteoarthritis. BMC Complement Altern Med. 2017;17(1). [Google Scholar] [Crossref]
- Sushma N, Shyamasundaran K, Prajeesh Nath E, Puthiyedath R. Integrative approach combining Ayurveda, counselling, Yoga and meditation with conventional management of Ankylosing Spondylitis - A case report. J Ayurveda Integr Med. 2022;13(1). [Google Scholar] [Crossref]
- Hegde M, Girisa S, Chetty B, Vishwa R, Kunnumakkara A. Curcumin Formulations for Better Bioavailability: What We Learned from Clinical Trials Thus Far?. ACS Omega. 2023;8(12):10713-10746. [Google Scholar] [Crossref]
- Kunnumakkara A, Hegde M, Parama D, Girisa S, Kumar A, Daimary U. Role of Turmeric and Curcumin in Prevention and Treatment of Chronic Diseases: Lessons Learned from Clinical Trials. ACS Pharmacol Transl Sci. 2023;6(4):447-518. [Google Scholar] [Crossref]
- Majeed A, Majeed S, Satish G, Manjunatha R, Rabbani S, Patil N. A standardized Boswellia serrata extract shows improvements in knee osteoarthritis within five days-a double-blind, randomized, three-arm, parallel-group, multi-center, placebo-controlled trial. Front Pharmacol. 2024. [Google Scholar] [Crossref]
- Maouche A, Boumediene K BC. Bioactive Compounds in Osteoarthritis: Molecular Mechanisms and Therapeutic Roles. Int J Mol Sci. 2024;25(21). [Google Scholar] [Crossref]
- Elgazar A, El-Domany R, Eldehna W, Badria F. 3-Acetyl-11-keto-β-boswellic Acid-Based Hybrids Alleviate Acetaminophen-Induced Hepatotoxicity in HepG2 by the Regulation of Inflammatory and Oxidative Stress Pathways: An Integrated Approach. ACS Omega. 2023;8(42):39490-510. [Google Scholar] [Crossref]
- Sairkar P, Sharma A, Shukla N. Estimation of Guggulsterone E and Z in Guggul-Based Commercial Formulations Using HPTLC. J Pharm Bioallied Sci. 2017;9(1). [Google Scholar] [Crossref]
- Kumar P, Sharma R, Garg N. Withania somnifera - a magic plant targeting multiple pathways in cancer related inflammation. Phytomedicine. 2022. [Google Scholar] [Crossref]
- Kulkarni R, Virkar AD DP. Antioxidant and Anti-Inflammatory Activity of Vitexnegundo. Indian J Pharm Sci. 2008. [Google Scholar] [Crossref]
- Peng C, Yang Y, Wang Y, Gong B, Sun X, Yang X. From Bench to Bedside: Boswellic Acids in Anti-Inflammatory Therapy. Front Pharmacol. 2025. [Google Scholar] [Crossref]
- Ghosh S, Solanki R, Bhatia D, Sankaranarayanan S. Nanomaterials for Delivery of Medicinal Plant Extracts and Phytochemicals. Plant Nano Biol. 2025. [Google Scholar] [Crossref]
- Koppula S, Shaik B, Maddi S. Phytosomes as a New Frontier and Emerging Nanotechnology Platform for Phytopharmaceuticals: Therapeutic and Clinical Applications. Phytother Res. 2025;39(5):2217-49. [Google Scholar] [Crossref]
- Yi X, Leng P, Wang S, Liu L, Xie B. Functional Nanomaterials for the Treatment of Osteoarthritis. Int J Nanomedicine. 2024;19:6731-56. [Google Scholar] [Crossref]
- Rahim M, Zahran H, Jaffar H, Ambreen S, Ramadan M, Al-Asmari F. Liposomal Encapsulation in Food Systems: A Review of Formulation, Processing, and Applications. Food Sci Nutr. 2025;13(8). [Google Scholar] [Crossref]
- Bakhrushina E, Shumkova M, Avdonina Y, Ananian A, Babazadeh M, Pouya G. Transdermal Drug Delivery Systems: Methods for Enhancing Skin Permeability and Their Evaluation. Pharmaceutics. 2025;17(7). [Google Scholar] [Crossref]
- Adepu S, Ramakrishna S. Controlled Drug Delivery Systems: Current Status and Future Directions. Molecules. 2021;26(19). [Google Scholar] [Crossref]
- Parasuraman S, Thing G, Dhanaraj S. Polyherbal formulation: Concept of ayurveda. Pharmacogn Rev. 2014;8(16):73-80. [Google Scholar] [Crossref]
- Sharma V, Jindal A, Sharma R. Ayurveda and Nanotechnology: A Synergistic Approach. J Ayurveda Integr Med Sci. 2025. [Google Scholar] [Crossref]
- Sun S, Wang Y, Wu A, Ding Z, Liu X. Pharmacokinetics of Herbal Compounds. Evid-Based Complement Altern Med. 2019. [Google Scholar] [Crossref]
- Dua P, Dua P. Recent Changes in Clinical Trials Regulatory Framework in India: AYUSH Sector. Int J Res Ayurveda Pharm. 2013. [Google Scholar] [Crossref]
- Bailey R, English J, Knee C, Keller A. Treatment Adherence in Integrative Medicine-Part One: Review of Literature. Integr Med (Encinitas). 2021;20(3):48-60. [Google Scholar]
- Mathur A, Sankar V. Standards of reporting Ayurvedic clinical trials - Is there a need?. J Ayurveda Integr Med. 2010;1(1):52-5. [Google Scholar] [Crossref]
- Chele K, Piater LA vdHJ, Tugizimana F. Bridging Ethnobotanical Knowledge and Multi-Omics Approaches for Plant-Derived Natural Product Discovery. Metabolites. 2025;15(6). [Google Scholar] [Crossref]
- Preethy H, Rajendran K, Mishra A, Karthikeyan A, Chellappan D, Ramakrishnan V. Towards understanding the mechanism of action of a polyherbal formulation using a multi-pronged strategy. Comput Biol Med. 2022. [Google Scholar] [Crossref]
- Ou J, Zhang J, Alswadeh M, Zhu Z, Tang J, Sang H. Advancing osteoarthritis research: the role of AI in clinical, imaging and omics fields. Bone Res. 2025;13(1). [Google Scholar] [Crossref]
- Wavhal P. . J Ayurveda Integr Med. 2025. [Google Scholar] [Crossref]
- 1. Introduction
- 1.1. Global prevalence and burden of osteoarthritis
- 1.2. Limitations of current therapeutic strategies
- 1.3. Rationale for integrative medicine
- 1.4. Scope and objectives of the review
- 2. Pathophysiology of Osteoarthritis
- 2.1. Articular cartilage degradation
- 2.2. Synovial inflammation and cytokine networks (IL-1β, TNF-α, IL-6)
- 2.3. Role of oxidative stress and reactive oxygen species (ROS)
- 2.4. Subchondral bone changes and osteophyte formation
- 2.5. Molecular pathways: NF-κB, MAPKs, Wnt/β-catenin
- 2.6. Genetic and epigenetic influences
- 3. Ayurvedic Perspective on Osteoarthritis
- 3.1. Understanding sandhigata vata
- 3.2. Etiopathogenesis: Vata vruddhi, dhatukshaya, and ama formation
- 3.3. Lakshanas (clinical symptoms) as defined in classics
- 3.4. Ayurvedic diagnostic considerations[20]
- 3.5. Comparative mapping of ayurvedic concepts to modern pathology
- 4. Current Pharmacotherapeutic Options in OA
- 4.1. NSAIDs and analgesics
- 4.2. Corticosteroids and intra-articular injections
- 4.3. Viscosupplements (hyaluronic acid)
- 4.4. DMOADs: Current status and limitations
- 4.5. Biologicals (IL-1 inhibitors, TNF-α blockers)
- 4.6. Safety issues, adverse drug reactions, and unmet clinical needs
- 5. Evidence-Based Ayurvedic Therapeutics
- 5.1. Internal medications
- 5.2. External therapies
- 5.3. Panchakarma interventions
- 5.4. Nutritional and lifestyle interventions (Āhāra–Vihāra)
- 5.5. Clinical evidence supporting ayurvedic treatment
- 6. Synergistic Potential
- 6.1. Conceptual synergy
- 6.2. Anti-inflammatory, antioxidant & chondroprotective convergence
- 6.3. Complementary benefits: Enhanced efficacy with fewer adverse effects
- 6.4. Herb–drug interactions
- 6.5. Evidence from integrative clinical models
- 7. Phytochemistry and Mechanisms of Key Ayurvedic Herbs
- 7.1. Boswellic acids and 5-LOX inhibition
- 7.2. Guggulsterones and anti-inflammatory pathways
- 7.3. Withanolides from ashwagandha
- 7.4. Flavonoids, terpenoids, and alkaloids in OA modulation.[48]
- 7.5. Preclinical and molecular docking insights
- 8. Discussion
- 8.1. Advances in modern drug delivery and ayurvedic integration
- 8.2. Nanotechnology-enabled drug delivery
- 8.3. Encapsulation of herbal phytoconstituents
- 8.4. Transdermal and topical novel systems
- 8.5. Controlled release formulations for chronic OA
- 8.6. Combining modern delivery with ayurvedic herbal extracts
- 9. Challenges in Integrative Osteoarthritis Management
- 9.1. Standardization of herbal raw materials
- 9.2. Quality control and GMP compliance
- 9.3. Dose optimization and safety monitoring
- 9.4. Regulatory challenges
- 9.5. Patient-centered barriers: Acceptability and adherence
- 10. Research Gaps and Future Directions
- 10.1. Need for robust randomized controlled trials (RCTs) on integrative OA protocols
- 10.2. Omics-based profiling of ayurvedic herbs
- 10.3. Systems biology approach for multi-target therapy
- 10.4. Digital therapeutics and AI for personalized disease management
- 10.5. Bridging traditional knowledge with pharmacological sciences
- 11. Conclusion
- 12. Source of Funding
- 13. Conflict of Interest
- References
Article Metrics
- Visibility 39 Views
- Downloads 17 Views
- DOI 10.18231/j.pharmacist.40990.1783398087
-
CrossMark

- Citation
- Received Date March 31, 2026
- Accepted Date May 02, 2026
- Publication Date July 07, 2026